A hernia occurs when an organ pushes through an opening in the muscle or tissue that normally holds it in place. For example, the intestines may break through a weakened area in the abdominal wall. Hernias are most common in the abdomen, but they can also appear in the upper thigh, belly button, and groin areas, or at the site of a prior surgical incision.
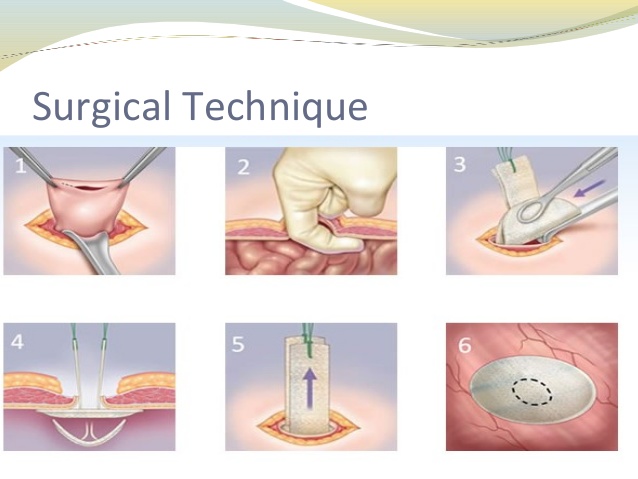
- Inguinal hernia An inguinal hernia occurs when tissue, such as part of the intestine, protrudes through a weak spot in the abdominal muscles of the groin. The bulge can be painful, especially when you cough, bend over or lift a heavy object, or sometimes even when doing nothing. An inguinal hernia isn’t necessarily dangerous, but it will not improve on its own, and can potentially lead to life-threatening complications. Not all inguinal hernias need to be repaired immediately, but those hernias that cause significant pain, or are increasing in size, or limiting the ability to perform normal duties, (household, work, recreational), should be repaired. Repair is accomplished by closing the weak spot in the abdominal muscles, usually with a small piece of mesh, and is an outpatient procedure.
- Ventral hernia–A ventral hernia occurs when tissue, usually the intestine, or fat inside the abdomen pushes through the muscle layer. When this occurs at the navel, it is termed an umbilical hernia, and if at the site of a previous surgery, the term is incisional hernia. These type of hernias may not cause any pain or discomfort when a person is lying flat, but may become painful/uncomfortable when standing, lifting, straining, or coughing. If a portion of intestine has protruded through, and becomes stuck, the result can be a blockage, (obstruction), and cause nausea/vomiting. In this event, immediate repair is necessary, otherwise the portion of intestine that is stuck may die, due to its blood supply being interrupted. Like inguinal hernias, a ventral hernia will not improve on its own, but not all hernias need immediate repair, and can be planned. A hernia that is causing significant discomfort, increasing in size, or requires repair to allow an individual to be able to perform physical activities requires for work/school should be repaired electively. As in the case of inguinal hernias, repair is performed by closing the weak/separated muscle, often with a mesh, if required. Usually, the surgery is performed as an outpatient but larger hernias may require an overnight stay in the hospital. In many cases, we perform the repair using a mesh laparoscopically.
- Hiatal hernia The hiatus is an opening in the diaphragm — the muscular wall separating the chest cavity from the abdomen. Normally, the esophagus (food pipe) goes through the hiatus and attaches to the stomach. In a hiatal hernia, the opening that allows passage of the esophagus is wider than normal and the stomach bulges up into the chest through that opening. Many people with hiatal hernia have no symptoms, but others may have heartburn related to gastroesophageal reflux disease, (GERD). If the hernia is large enough and a large portion of the stomach is in the chest, symptoms may include chest pain and shortness of breath, or feelings of food getting stuck in the lower chest. Some patients develop ulcerations in the portion of the stomach that protrudes into the chest. In the majority of patients with reflux as the main symptom, management is usually with antacids; however, if reflux persists despite medication, or if chest pain, shortness of breath, and feeling of food getting stuck are present, often we will recommend surgery. The surgery performed is called a Nissen Fundoplication, and involves:
- Closing the opening in the diaphragm to allow only the esophagus to pass, and
- Wrapping the floppy upper portion of the stomach, (the fundus) around the lower esophagus to prevent it from moving back into the chest.This surgery is done laparoscopically in most cases and involves an overnight stay in the hospital.