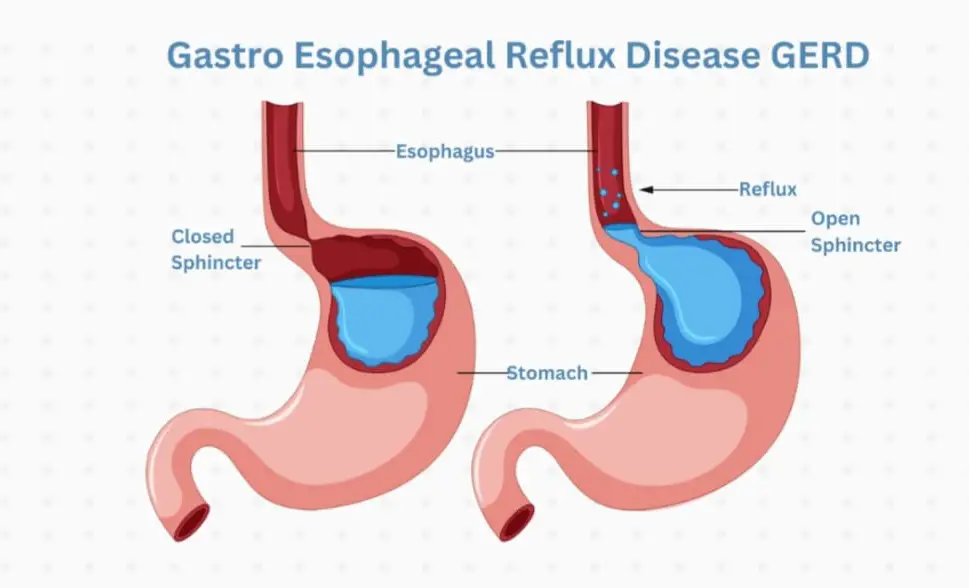
Anti-reflux surgery is a treatment for acid reflux, also known as GERD (gastroesophageal reflux disease). Patients may also have a hiatal hernia in addition to having GERD. GERD is a condition in which food or stomach acid comes back up from your stomach into the esophagus. The esophagus is the tube from your mouth to the stomach.
Reflux often occurs if the muscles where the esophagus meets the stomach do not close tightly enough. A hiatal hernia can make GERD symptoms worse. It occurs when the stomach bulges through this opening into your chest.
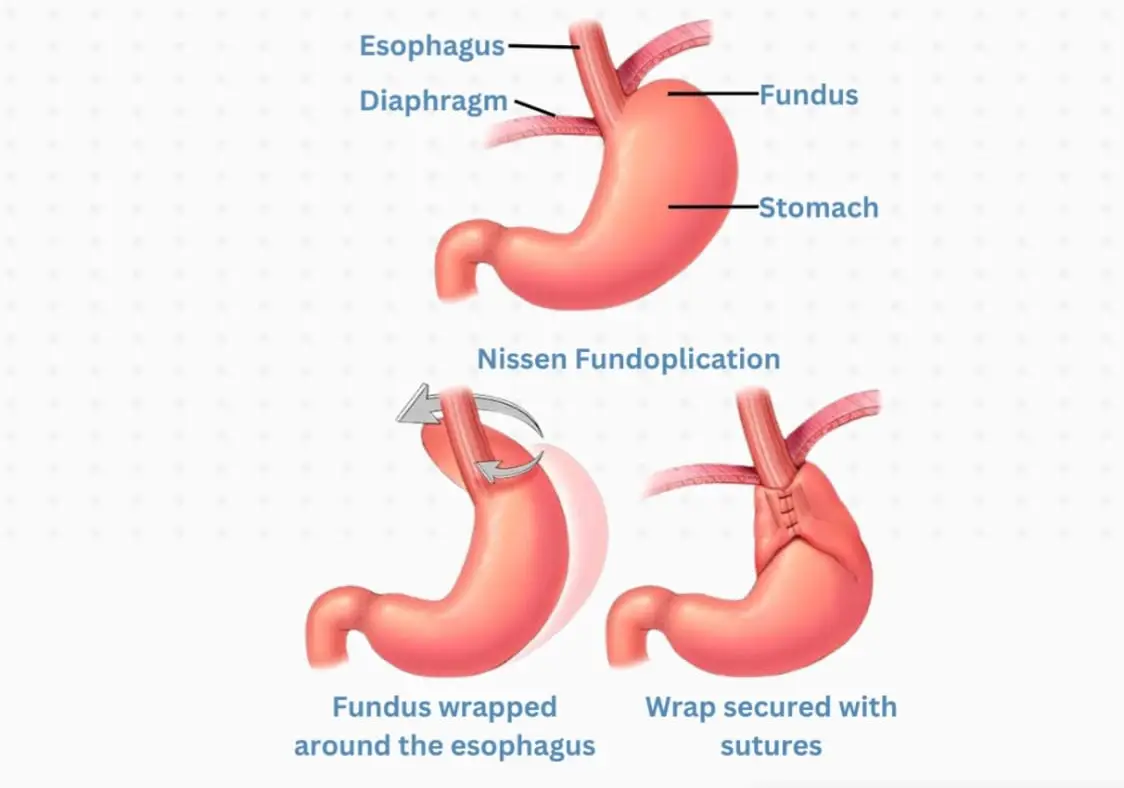
The most common procedure of this type is called fundoplication. In this surgery, your surgeon will:
⦁ First repair the hiatal hernia, if one is present. This involves tightening the opening in your diaphragm with stitches to keep your stomach from bulging upward through the opening in the muscle wall. Sometimes, if large enough, we place a piece of mesh in the repaired area to make it more secure.
⦁ Wrap the upper part of your stomach around the end of your esophagus with stitches. The stitches create pressure at the end of your esophagus, which helps prevent stomach acid and food from flowing up from the stomach into the esophagus.
Surgery is done while you are under general anesthesia, so you are asleep and pain-free. Surgery most often takes 1.5 to 2 hours. Your surgeon may choose from different techniques.
⦁ Your surgeon will make 1 large surgical cut in your belly.
⦁ A tube may be inserted into your stomach through the abdomen to keep the stomach wall in place. This tube will be taken out in about a week.
⦁ This method is rare and usually only performed in severe emergencies.
⦁ Your surgeon will make 4 to 5 small cuts in your belly. A thin tube with a tiny camera on the end is inserted through one of these cuts.
⦁ Surgical tools are inserted through the other cuts. The laparoscope is connected to a video monitor in the operating room.
⦁ Your surgeon does the repair while viewing the inside of your belly on the monitor.
⦁ The surgeon may need to switch to an open procedure in case of problems.
Before surgery is considered, your health care provider will have you try:
Surgery to treat your heartburn or reflux symptoms may be recommended when:
⦁ Your symptoms do not get much better when you use medicines.
⦁ You do not want to keep taking these medicines.
⦁ You have more severe problems in your esophagus, such as scarring or narrowing, ulcers, or bleeding.
⦁ You have reflux disease that is causing aspiration pneumonia, a chronic cough, or hoarseness.
Risks of any anesthesia and surgery in general are:
Risks of this surgery are:
⦁ Damage to the stomach, esophagus, liver, or small intestine. This is very rare.
⦁ Gas bloat. This is when the stomach overfills with air or food and you are unable to relieve the pressure by burping or vomiting. These symptoms slowly get better for most people.
⦁ Pain and difficulty when you swallow. This is called dysphagia. In most people, this goes away during the first 3 months after surgery.
⦁ Return of the hiatal hernia or reflux.
Before the Procedure:
You may need the following tests:
Before your surgery:
⦁ You may need to stop taking aspirin, ibuprofen (Advil, Motrin), vitamin E, clopidogrel (Plavix), warfarin (Coumadin), and any other drugs or supplements that affect blood clotting several days before surgery.
After the Procedure
Most people who have laparoscopic surgery can leave the hospital the same day or the next day.
Outlook (Prognosis)
Heartburn and other symptoms should improve after surgery. The majority of patients will be able to stop taking their antacid after surgery. Similar to other hernias, the widening in the muscle occurs because of tension and the muscle is weak. It is possible that the hernia may recur; however, this is much less likely for hiatal hernia than for hernias in other parts of the body.
© 2025, Rath Surgical Group | All rights reserved.